
There is a lot of patient anxiety surrounding thyroid biopsies. I myself am a bit of a needle phobe and even dread my annual flu shot. That being said I think there are a lot of misconceptions, mixed with poor technique, as well as outmoded procedures performed by many clinicians. As I discussed in my last post, I cannot stress enough to seek care by a dedicated thyroidologist or interventional thyroidologist for your thyroid care and in this case a thyroid biopsy. I get anxious questions and concerns about thyroid biopsies on a daily basis, especially from patients who have had a history of previous biopsy.
Most of these misconceptions are a result of outdated techniques, improper tools, and surprisingly, sometimes still the wrong procedure. Technically the procedure I favor is called a fine needle aspiration or (FNA). Shockingly, I still know of institutions that still perform core needle biopsies. A thyroid FNA is a procedure where a very small needle is used to get a small sample of thyroid cells which are then submitted to pathology for review. A core biopsy is when a larger needle is used to obtain a fragment of tissue. When I perform a thyroid FNA I use a 27 gauge needle, essentially the smallest that I can reasonably obtain in the commercial setting for the purpose of FNA. A core biopsy typically uses an 18-21 gauge needle. For comparison see the image below.

An 18 gauge needle is about 3 TIMES the diameter of a 27 gauge needle, This makes a HUGE difference. There is somewhat mixed literature regarding the use of a core biopsy over FNA, mostly surrounding large thyroid nodules, and there is some discussion regarding obtaining a core biopsy in the setting of a non-diagnostic FNA (an FNA with an insufficient sample to make a diagnosis) but in the hands of a skilled Interventional Thyroidologist a patient can expect a non-diagnostic rate of less than 5%, and in many cases less than 1%. Since my non-diagnostic rate is less than one per year, I don’t see much of a role for core biopsy in my practice.
Not only do some institutions still perform a core biopsy they also use an approach that is less comfortable for the patient. We briefly discussed a thyroid ultrasound in the last post in that it uses sound waves to create an image of structures in the body, in our case of the neck. Below is an image of a thyroid ultrasound picture of the anterior neck and a diagram of the neck anatomy as viewed by a thyroid ultrasound in the transverse (left to right) view.

The point of the diagrams is not to make you an expert in neck anatomy but to note that there are a lot of muscle and soft tissue structures laterally (to the side) of the thyroid gland itself and there is little soft tissue or musculature superior (above) the thyroid in that view.
With the basic neck anatomy in mind, it should be noted that there are generally two ways that a thyroid biopsy can be performed. The needle can be passed in plane (parallel) to the sound waves from the ultrasound or out of plane (perpendicular) to the sound wave from the transducer. The major advantage of the parallel approach is the needle is readily visualized from skin to target but it must pass through a lot more soft tissue to reach its target (especially if it is inserted laterally to the target structure). The major advantage of the perpendicular approach is that it passes through minimal soft tissue from skin to target, but the needle cannot be visualized along the entire path and as such requires an experienced clinician to perform the procedure using this technique.
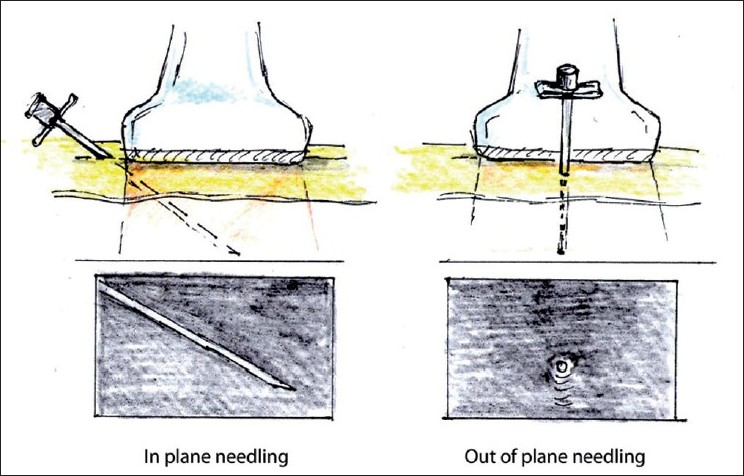
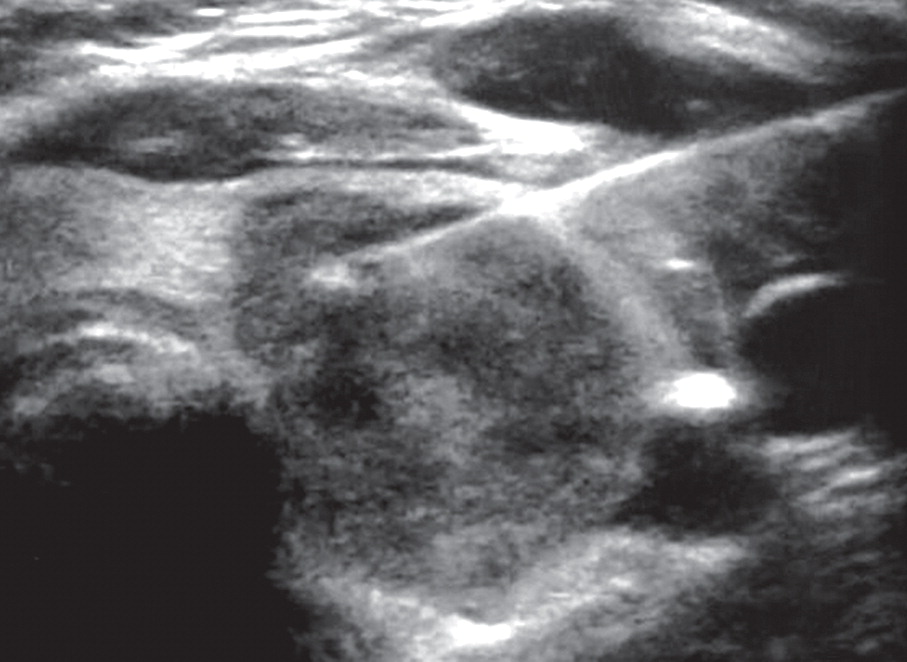
The most common technique that I see from imaging centers, radiologists, and even ENT is the parallel approach with a relatively large gauge needle with the insertion lateral to the target which often results in significant discomfort as well as bruising. One need only google bruising after thyroid biopsy to see the results of the procedure likely done this way. Below is an image of a parallel, in plane, approach to a thyroid nodule with a lateral approach. Note the amount of muscle and soft tissue through which the needle must pass to reach its target. Compared to if a perpendicular approach (out of plane) technique was used as in the second picture. I can tell from this ultrasound image that this patient was not positioned correctly, at least not for a perpendicular approach as the neck should be extended back to aid the procedure. The amount of tissue would be even less if this patient were positioned correctly (neck extended which pulls the thyroid up closer to the surface of the skin and pulls the overlying musculature
laterally and less in the way).

As a patient, you would much prefer the approach with the least amount of discomfort that still results in appropriate diagnostic material. As such, you should pursue an FNA with the smallest needle possible (27 gauge needle), and an approach from above the thyroid (out of plane or perpendicular), with appropriate patient positioning, by an experienced interventional thyroidologist. Smaller needle, less discomfort, excellent diagnostic results. The next post will discuss what to expect at your biopsy appointment.

Dr. Shahzad Ahmad
The Thyroid Clinic
Salt Lake City, Utah
www. thyroidradiofrequency.com